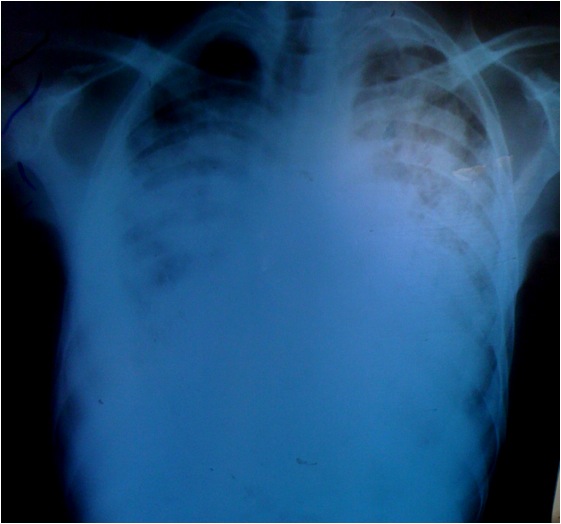
History: A 40 year old male with c\o fever, cough productive of mucoid sputum without haemoptysis and chest pain for four months. He also reported weight loss for two months and abdominal and lower limb swelling for one month. In addition he had fatigue, palpitations and exertional dyspnoea but denied orthopnoea. Chest X-ray showed a massively enlarged cardiac silhouette and bilateral pulmonary infiltrates or oedema. An urgent bedside ultrasound showed a large pericardial effusion of about 2 cm, right atrial collapse and right ventricular collapse in diastole. What’s the diagnosis?
Answer: The patient presented with cardiac tamponade, the most severe complication of TB pericarditis. Cardiac tamponade occurs when fluid in the pericardial space accumulates faster than the pericardial sac can stretch and so causes high pressure compressing the heart and preventing the heart from expanding fully. However, if the fluid accumulates more slowly as with TB pericarditis, the pericardial sac can expand to hold over one litre of fluid before critical compression arises.
Signs & Symptoms: The three classical signs of cardiac tamponade (Beck’s triad) are hypotension, jugular venous distention, and muffled heart sounds. Hypotension results from decreased cardiac output, jugular-venous distension results from impaired venous return to the heart and, muffled heart sounds are due to pericardial fluid. There are other physical signs that may indicate cardiac tamponade. On inspiration the central venous pressure (jugular venous pressure) would normally fall but with tamponade this rises. Pulsus paradoxus is the finding of a fall in the systolic blood pressure of more than 10mmHg when the patient inspires.
Causes: Infection- viral, TB, bacterial, fungal, HIV, Malignancy, Post-cardiac injury syndrome (after trauma or cardiothoracic surgery), Acute myocardial infarction (acute, delayed), Metabolic-uremia, hypothyroidism, Collagen vascular diseases- rheumatoid arthritis, lupus erythematosus, Radiation, Idiopathic.
Investigation: The chest Xray of a patient with large pericardial effusion shows a large “boot-shaped” cardiac silhouette but it can be difficult to tell if a large heart is due to dilated cardiomyopathy or pericardial effusion. Ultrasound easily detects a large pericardial effusion: the fluid appears anechoic or black around the heart. The right atrium and right ventricle appear collapsed with dilation of the inferior vena cava.
Treatment: Emergency pericardiocentesis by a subxiphoid approach using ultrasound guidance.