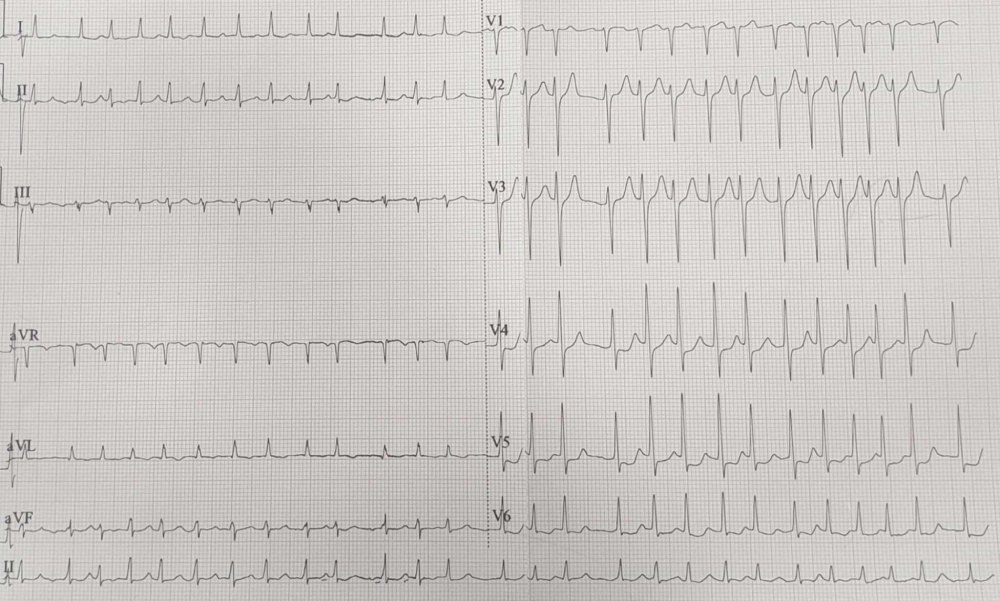
History: A 67-year-old male k/c/o CKD-5 on MHD thrice weekly with Type2DM & HTN presented to ED with SOB, anasarca and AMS. P – 164 bpm irregular, SP02- 80 % on RA, RR – 30, R/E – B/L AE ↓ with B/L crepitations +nt. E3V2M5. ABG – pH 7.17, pCO2 9.7, Na+ 135, k+ 4.5, Lac 10.7, Glu 141, HCO3- 3.6. ECG was done. What’s the diagnosis?
Answer: ECG shows irregularly irregular narrow complex tachycardia with absent P waves & ST ↓ V4-V6 which is s/o Atrial fibrillation.
Classification is dependent on the presentation and duration of atrial fibrillation as below:
First episode – initial detection of AF regardless of symptoms or duration
Recurrent AF – More than 2 episodes of AF
Paroxysmal AF – Self-terminating episode < 7 days
Persistent AF – Not self-terminating, duration > 7 days
Long-standing persistent AF – > 1 year
Permanent AF – Duration > 1 yr in which rhythm control interventions are not pursued or are unsuccessful.
How will you manage the above patient in the ED? Write down in the comment section.