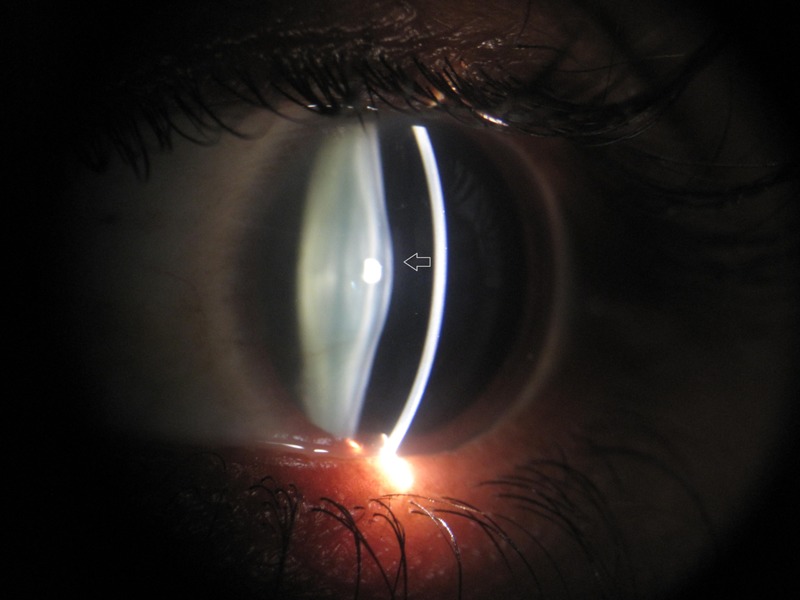
History: A 33-year-old man presented to the ED with low-grade fever for 3 weeks, vomiting for 1 week and anuria for 3 days. He also reported dysuria and breathlessness for 1 week. There was no history of decreased urine output, dialysis, effort intolerance, chest pain or palpitation, dyspnoea and weight loss. Family history included smoky urine in his younger brother in his childhood. Severe pallor was present with mild pedal oedema. BP 180/100 mm Hg and P 116/min regular. No evidence of jaundice, clubbing cyanosis or lymphadenopathy was found. Physical examination revealed bibasilar end-inspiratory crepitations in lungs and suprapubic tenderness. There was no hepatosplenomegaly or ascites. Cardiac examination was normal. He was found to have severe bilateral hearing loss, which was gradually progressive for 5 years. Slit-lamp examination showed bilateral anterior lentiglobus with posterior lenticonus. What’s the diagnosis?
Answer: Alport syndrome is caused by mutations in COL4A3, COL4A4, and COL4A5, three of six human genes involved in basement membrane (type IV) collagen biosynthesis.
Signs & symptoms: Hereditary nephritis, sensorineural hearing loss, retinopathy, anterior lenticonus.
Diagnosis: At least 4 of the following 10 criteria should be fulfilled:
- A family history of nephritis in a first-degree relative male linked to the index case.
- A history of persistent haematuria.
- Bilateral SNHL involving higher frequencies.
- Widespread GBM ultrastructural abnormalities.
- Ocular findings such as anterior lenticonus and retinal flecks.
- Mutation in COL4A gene.
- Immunohistochemical evidence of partial or complete loss of Alport epitope.
- Gradual progression to ESRD in at least relatives of index case.
- Macrothrombocytopenia.
- Diffuse leiomyomatosis.
Differential diagnosis: Thin basement membrane disease (TBMD), Mesangial IgA nephropathy, Drug-induced renal and ototoxicity (eg, aminoglycosides), Branchio-otorenal syndrome.
Treatment: ACE inhibitors, dialysis or transplantation.